
Report on the History and Current Research Against Cancer
Introduction
Cancer, defined as a group of diseases characterized by the abnormal and uncontrolled proliferation of cells, represents one of the leading causes of global mortality. Since its first descriptions in antiquity, cancer research has evolved from empirical approaches to molecular and personalized strategies. This report presents a structured history of this fight, followed by an overview of advances in 2026 and a detailed analysis of key areas, challenges, and perspectives. The information is based on reliable scientific and institutional sources, highlighting continuous progress in prevention, diagnosis, and treatment.
I. History of Cancer Research
The presence of cancer is attested since prehistory, with traces on human bones dating back 120,000 years and even in dinosaurs over 76 million years ago. The first written descriptions date back to Ancient Egypt, where the Edwin Smith Papyrus (circa 2800 BC) mentions incurable breast tumors treated by cauterization. Over the centuries, concepts have evolved from humoral theories to cellular and genetic approaches.
Evolution of Concepts and Key Discoveries
- Antiquity (circa 525 BC - 2nd Century AD): Hippocrates (460-370 BC) introduced the term "carcinoma" due to the crab-like appearance of tumor veins and classified tumors based on their location (breast, stomach, uterus). Galen (130-201 AD) attributed cancer to an excess of black bile and advocated purges or excisions.
- Middle Ages and Arab Medicine (10th-12th Centuries): Avicenna (980-1037) described the slow progression of tumors with tissue invasion. Albucasis (1013-1106) recommended early excision and cauterization of margins for accessible lesions.
- Renaissance and Modern Era (16th-18th Centuries): Systematic autopsies, initiated by Morgagni (1682-1771), founded anatomical pathology. Percival Pott (1714-1788) identified the first occupational cancer in 1775 (chimney sweeps' scrotal cancer due to soot). Le Dran (1685-1770) described lymphatic dissemination, advocating lymph node removal.
- 19th-20th Centuries: The cellular theory emerged with Virchow (1821-1902), who demonstrated that cancer cells originate from other abnormal cells. Récamier (1829) introduced the concept of "metastasis." The discoveries of Röntgen (X-rays, 1895) and the Curies (radium, 1898) laid the foundations for radiotherapy. In the 20th century, Yamagiwa (1915) induced the first experimental cancer in animals, confirming the role of chemical carcinogens. Ehrlich (1910s) pioneered chemotherapy.
Timeline of Key Milestones (France & International)
Research became institutionalized in the 20th century, with national plans and dedicated organizations. Here is a summary timeline of major milestones:
| Date | Main Event | Impact |
|---|---|---|
| 2800 BC | Edwin Smith Papyrus: First description of breast tumors in Egypt. | Early clinical recognition. |
| 460-370 BC | Hippocrates: Classification of carcinomas and rejection of magical theories. | Foundations of rational medicine. |
| 1895 | Discovery of X-rays by Röntgen. | Initiation of radiotherapy (1904). |
| 1898 | Discovery of radium by Pierre and Marie Curie. | Advances in brachytherapy (curietherapy). |
| 1918 | Foundation of the League against Cancer in France. | Institutional mobilization. |
| 1915-1921 | Yamagiwa: First chemically induced cancer in rabbits. | Proof of the role of carcinogens. |
| 1940s | Development of chemotherapy (mustard gas derivatives). | Systemic treatments. |
| 1950s | Higgins: Hormonal role in female cancers. | Hormone therapy. |
| 1971 | "War on Cancer" declared by Nixon (USA). | Massive increase in funding. |
| 2003 | First Cancer Plan in France (Chirac). | Integrated national strategies. |
| 2009 | Second Cancer Plan (Sarkozy); Focus on translational research. | Acceleration of clinical trials. |
| 2014 | Third Cancer Plan (Hollande); Emphasis on immunotherapy. | Integration of genomics. |
| 2021-2025 | Fourth Cancer Plan; AI and personalized medicine. | Preparation for 2026-2030 plans. |
II. Current Advances in Cancer Research (Status in 2026)
In 2026, research marks a turning point towards the integration of artificial intelligence (AI), adaptive medicine, and targeted therapies, with a global five-year survival rate exceeding 70% for the first time in some countries. World Cancer Day (February 4, 2026) focused on AI, revealing that 77% of French people see its role as essential in personalized care, despite a lack of awareness.
Technological and Therapeutic Progress
- Genomics and Liquid Biopsies: Single-cell analyses map tumor heterogeneity, allowing real-time monitoring via circulating tumor DNA to detect early resistance. In France, advances in ferroptosis (iron-dependent cell death) target refractory cells.
- Immunotherapy and Cell Therapies: Expansion of "armored" CAR-T cells (expressing IL-18 or IL-12) for increased persistence in tumor microenvironments. RNA vaccines against "dark" antigens (alternative DNA readings) for pancreatic cancers. In 2025-2026, combinations with chemotherapy and checkpoint inhibitors show durable responses.
- Artificial Intelligence: Used in radiomics to identify the origin of cancers in 80% of unknown primary cases; prediction of therapeutic responses and clinical decision support. AI accelerates drug design via protein modeling and clinical trial matching.
- Prevention and Screening: "Interception" strategies for precancerous conditions (e.g., prostatic intraepithelial neoplasia). Non-invasive tests (blood, stool) for colorectal cancer, with AI reducing false positives in lung imaging. Focus on obesity (linked to 13 cancers) via GLP-1 agonists.
The 2026-2030 Cancer Strategy in France accelerates prevention, research, and equity, with a reinforced budget for clinical trials.
III. Detailed Report: Areas, Challenges, and Perspectives
Main Research Areas
- Precision Medicine: Integration of proteomics, RNA sequencing, and digital pathology to phenotype tumors (e.g., glioblastomas, sarcomas). Use of PROTACs to target mutated KRAS in pancreatic cancers.
- Immuno-Oncology: Bispecific therapies (e.g., for gastroesophageal cancers) and combined lipoplex vaccines.
- Adaptive Radiotherapy: Real-time adjustments via imaging to minimize damage to healthy tissues.
- Equity and Disparities: Extension of mobile screening (low-dose CT for lungs) in underserved communities; expanded germline genetic testing.
Major Challenges
- Resistance and Heterogeneity: Tumors evolve, requiring adaptive approaches; only 50% of patients are integrated into clinical trials.
- Ethics of AI: Sharing of sensitive data and algorithmic biases; 60% of young French people perceive AI as a "gadget."
- Global Access: In Francophone Africa, pediatric cancers represent 4-6% of cases versus 0.5% in the West, due to infectious factors. High costs of innovative therapies.
Future Perspectives
Towards 2030, AI and liquid biopsies could reduce recurrences by 30% via detection of microscopic residual disease. National plans aim for total personalization, with preventive vaccines and gene therapies. International collaboration (e.g., UICC) will accelerate technology transfers.
Detailed Report on Immunotherapy in Cancer Treatment
Introduction
Immunotherapy represents a revolutionary therapeutic approach that harnesses the patient's immune system to fight cancer cells. Unlike conventional treatments such as chemotherapy or radiotherapy, which directly target tumors, immunotherapy stimulates or restores the body's natural defenses, often offering durable responses in certain patients. Emerging clinically in the early 2010s, it has transformed the management of various cancers, such as melanoma, lung cancer, and lymphomas. In 2026, its advances highlight growing potential for personalized medicine, although challenges remain regarding efficacy and accessibility.
Mechanisms of Action
The immune system plays a central role in antitumor surveillance via a process called immuno-editing, which occurs in three phases: elimination (early destruction of abnormal cells), equilibrium (latent control of the tumor), and escape (emergence of resistant cells). Cancer cells often exploit immune evasion mechanisms, such as the expression of inhibitory molecules (PD-L1) or the creation of an immunosuppressive microenvironment.
Immunotherapy intervenes to counter these evasions by:
- Activating Effector Cells: Primarily cytotoxic T lymphocytes (CD8+), which recognize and lyse tumor cells via antigens presented by the major histocompatibility complex (MHC).
- Inhibiting Checkpoints: Blocking pathways like PD-1/PD-L1 or CTLA-4 to lift immune brakes.
- Amplifying the Adaptive Response: By genetically modifying immune cells or administering specific antigens for targeted recognition.
These mechanisms enable long-term immune memory, explaining the prolonged remissions observed in some patients.
Types of Immunotherapies
Immunotherapies are classified into several categories, each adapted to specific tumor profiles:
| Type | Description | Application Examples | Main Mechanism |
|---|---|---|---|
| Immune Checkpoint Inhibitors | Monoclonal antibodies blocking inhibitory receptors on T lymphocytes. | Pembrolizumab (anti-PD-1) for melanoma and non-small cell lung cancer. | Release of T-cell response by inhibiting PD-1/CTLA-4. |
| Cell Therapies (CAR-T) | Genetic modification of the patient's T lymphocytes to express chimeric antigen receptors (CAR), directed against tumor markers. | Axi-cel for diffuse large B-cell lymphomas. | Direct recognition and destruction of target cells. |
| Therapeutic Vaccines | Administration of tumor antigens (proteins, messenger RNA, or dendritic cells) to stimulate a specific immune response. | Personalized vaccines based on tumor sequencing. | Activation of antigen-presenting cells for an adaptive response. |
| Immunomodulators | Agents globally stimulating immunity, such as interleukins or interferon. | IL-2 for renal carcinoma. | Increase in proliferation and activity of lymphocytes. |
| Antibody-Drug Conjugates (ADCs) | Antibodies linked to toxins or radioisotopes, targeting tumor antigens while activating immunity via ADCC (antibody-dependent cellular cytotoxicity). | Brentuximab vedotin for Hodgkin lymphoma. | Targeted destruction combined with immune activation. |
Recent Advances in 2026
The year 2026 marks an acceleration of innovations in immunotherapy, with a focus on personalization and extension to solid tumors. Notable progress includes:
- Innovative Monoclonal Antibodies: Montreal researchers have developed antibodies targeting SLAMF6, a molecule that inhibits T cells in the tumor microenvironment. These antibodies increase human T-cell activation and tumor destruction, opening pathways for combined therapies.
- Personalized Vaccines: A Geneva study demonstrates the efficacy of a therapeutic vaccine based on messenger RNA, successfully tested in humans for advanced cancers, inducing a robust immune response against neoantigens. In France, advances at the Institut Curie aim to adapt CAR-T cells for solid tumors, such as glioblastoma, making these therapies accessible beyond hematological cancers.
- Chronobiology and Optimization: Works reveal that immunotherapy is more effective for lung cancer if administered before 3:00 PM, in synchrony with circadian rhythms, highlighting the importance of temporal protocols.
- Emerging Strategies: Chinese molecules transform cancer cells into immune targets by exploiting antiviral memory, while next-generation therapies integrate AI to predict responses. Globally, experts foresee an increased focus on prevention and early detection, with personalized anti-cancer vaccines in advanced clinical phases.
Major Challenges
- Unusual Toxicities: In 10 to 50% of patients, it causes severe autoimmune reactions (cytokine release syndrome, colitis, pneumonitis), requiring increased monitoring.
- Variable Efficacy: Only 20-30% of patients respond durably, due to tumor heterogeneity and acquired resistance. "Cold" tumors (poor in lymphocyte infiltration) pose a particular challenge.
- Costs and Accessibility: Treatments like CAR-T often exceed 400,000 euros per patient, limiting their availability, especially in developing countries.
- Ethical and Regulatory Challenges: The integration of AI for personalization raises questions about bias and data privacy.
Detailed Report on CAR-T Therapies in Cancer Treatment
Introduction
CAR-T therapies (Chimeric Antigen Receptor T-cell therapy) constitute an advanced form of adoptive immunotherapy. They involve the genetic modification of the patient's T lymphocytes to equip them with an artificial receptor capable of recognizing and eliminating cancer cells in a targeted manner. First approved by the FDA in 2017 for refractory leukemias and lymphomas, these therapies have revolutionized the management of hematological malignancies, offering complete remissions in up to 80% of refractory patients. In 2026, their extension to solid tumors and autoimmune diseases marks a decisive step, although logistical and toxicity challenges persist.
Mechanisms of Action
CAR-T therapies rely on precise cellular engineering to bypass tumor cell immune evasion mechanisms. The process unfolds in several stages:
- Collection and Genetic Modification: T lymphocytes are extracted from the patient's
blood via leukapheresis. In the laboratory, a viral vector (usually a lentivirus) inserts a gene
coding for the CAR receptor, composed of:
- An extracellular domain (scFv) recognizing a specific tumor antigen (e.g., CD19 for B lymphomas).
- A transmembrane hinge and intracellular signaling domains (CD3ζ, CD28, or 4-1BB) to activate proliferation and cytotoxicity.
- Expansion and Re-injection: Modified cells are multiplied ex vivo (up to billions) and re-administered to the patient after lymphodepleting chemotherapy to favor their engraftment.
- In Vivo Action: CAR-T cells bind to the target antigen, triggering cytokine release (IL-2, IFN-γ), clonal proliferation, and lysis of tumor cells via granzymes and perforins. Immune memory can persist, conferring long-term protection.
Types and Applications (Generations)
CAR-T therapies are categorized into successive generations, adapted to specific indications:
| Generation | Key Characteristics | Approved Applications (2026) | Product Examples |
|---|---|---|---|
| 1st Generation | Basic signaling (CD3ζ alone); limited response. | Limited; historical phase. | - |
| 2nd Generation | Addition of a co-signal (CD28 or 4-1BB) for increased persistence. | Pediatric Acute Lymphoblastic Leukemia (ALL); Refractory Diffuse Large B-Cell Lymphoma (DLBCL). | Kymriah® (tisagenlecleucel); Yescarta® (axicabtagène ciloleucel). |
| 3rd Generation | Two co-signals (e.g., CD28 + 4-1BB); reduction of exhaustion. | Relapsed Multiple Myeloma; Follicular Lymphomas. | Tecartus® (brexucabtagène autoleucel); Breyanzi® (lisocabtagène maraleucel). |
| 4th Generation | "Armored" with cytokines (IL-12, IL-18) or safety switches; Allogeneic (from donors). | Trials for solid tumors (glioblastoma, pancreas); Autoimmune diseases (multiple sclerosis). | ALLO-501A (Allogene); Descartes-08 (CRISPR Therapeutics). |
In 2026, more than 10 products are approved worldwide, primarily for hematological cancers. Extensions to solid tumors target antigens such as HER2 or GD2.
Recent Advances in 2026
The year 2026 witnesses rapid maturation of CAR-T therapies, with a focus on allogeneic solutions, toxicity reduction, and therapeutic extension.
- First Non-Oncological Applications: At the CHU de Québec, a Canadian first uses CAR-T to treat primary progressive multiple sclerosis, reprogramming T cells to target auto-reactive B lymphocytes, with encouraging preliminary results on lesion reduction. In the US, trials for systemic lupus erythematosus show remission in 57% of patients at six months.
- Improvements for Solid Tumors: At the Institut Curie, CAR-T cells adapted for glioblastomas integrate cytokine "armor" to overcome immunosuppressive microenvironments, with partial responses in Phase I trials. Dr. Marco Davila (Roswell Park) presents findings on CAR-T resistance at Tandem 2026, identifying pathways for multi-target constructs reducing tumor escape.
- Allogeneic Products and Optimization: Allogene Therapeutics launches a pivotal trial for ALLO-501A in DLBCL in 2026, testing doses starting from 20 million cells, with "off-the-shelf" production to accelerate access. In Luxembourg, the CHL accredits CARVYKTI® for multiple myeloma, marking European expansion. A Memorial Sloan Kettering study reveals that morning administration (before 3:00 PM) optimizes efficacy via circadian rhythms.
Major Challenges
- Acute and Chronic Toxicities: Cytokine Release Syndrome (CRS, grade 3-4 in 10-20% of cases) and neurological syndrome (ICANS) require intensive care units. Rare cases of cell exhaustion limit persistence.
- Logistics and Costs: Personalized production takes 3-4 weeks and costs 300,000 to 500,000 euros per treatment, hindering access in under-equipped regions. The T2EVOLVE project identifies regulatory barriers in Europe.
- Resistance and Heterogeneity: Loss of target antigen (e.g., CD19) or "cold" tumor microenvironments reduce efficacy to 40-50% in solid tumors.
Future Perspectives
By 2030, CAR-T therapies could integrate hybrid approaches: universal allogeneic cells for immediate availability, combinations with checkpoint inhibitors, and use of AI to predict responses via biomarkers. Genes like those identified by the Salk Institute could reverse T-cell exhaustion, making therapies "unstoppable." The EBMT-EHA 2026 meeting will accelerate collaborations for Ewing sarcomas and solid tumors. In France, the 2026-2030 Cancer Plan will prioritize early interception and equity, potentially reducing hematological mortalities by an additional 25%.
Detailed Report on TIL Immunotherapies for Solid Tumors
Introduction
Tumor-Infiltrating Lymphocyte (TIL) therapies represent a form of personalized adoptive immunotherapy particularly adapted for solid tumors. Unlike CAR-T therapies, which are genetically modified to target a single antigen, TILs exploit T lymphocytes naturally present in the tumor that are already specific to tumor neoantigens. This approach, developed since the 1980s by Steven Rosenberg at the National Cancer Institute (NCI), achieved major validation with the FDA approval in February 2024 of lifileucel (Amtagvi®, Iovance Biotherapeutics), the first cellular treatment for a solid tumor (advanced melanoma). In 2026, real-world data and ongoing trials confirm its potential to expand indications to lung, head and neck, and other refractory solid tumors.
Mechanisms of Action
TILs are CD8+ and CD4+ T lymphocytes naturally infiltrating the tumor, recognizing neoantigens derived from somatic mutations. Their efficacy relies on:
- Polyclonal Recognition: Targeting multiple tumor antigens, reducing the risk of antigenic escape.
- Persistent In Vivo Activation: Favored by ex vivo expansion with interleukin-2 (IL-2) and prior lymphodepletion (non-myeloablative chemotherapy).
- Direct Cytotoxic Response: Via the release of perforins and granzymes, complemented by cytokine secretion (IFN-γ, TNF-α) amplifying antitumor inflammation.
This process exploits natural immune memory, offering durable responses in responding patients.
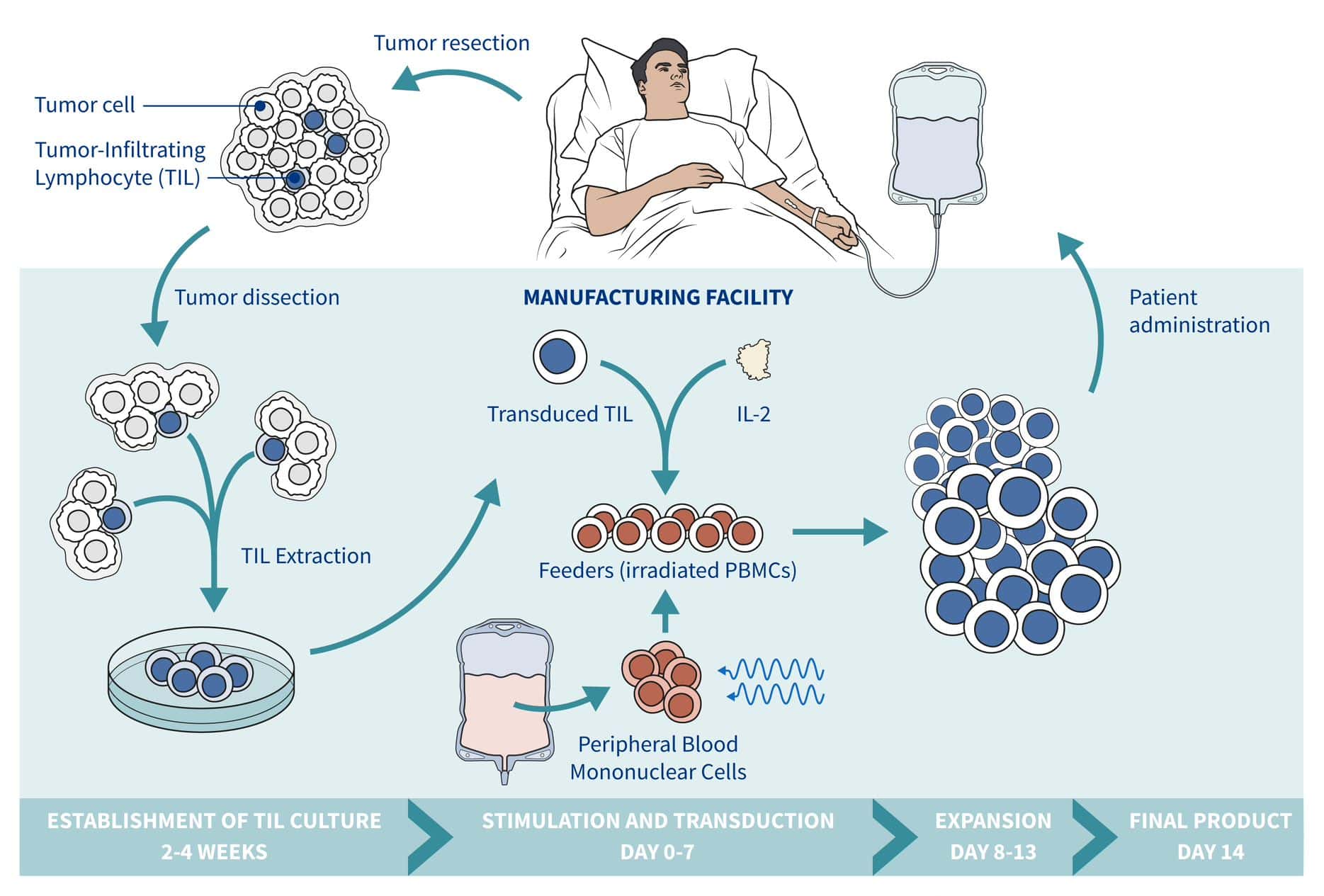
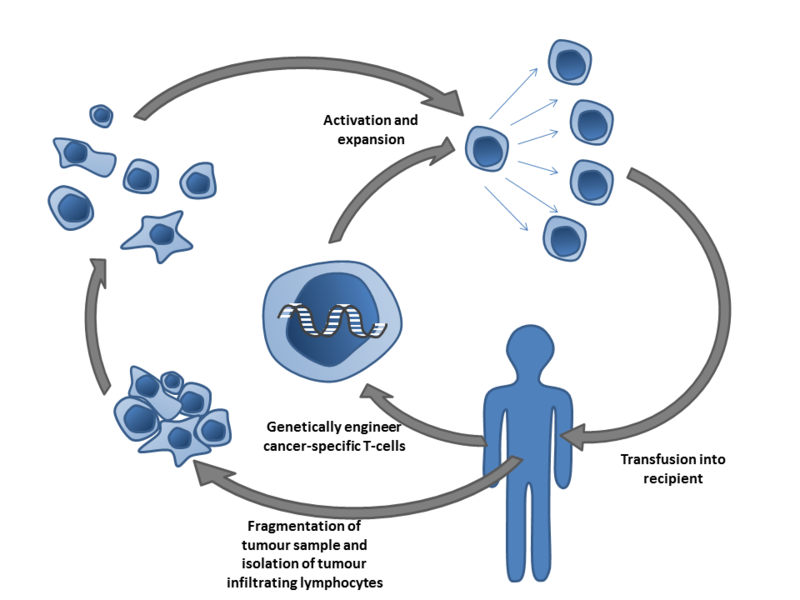
Therapeutic Process
The treatment follows a standardized protocol over 4 to 6 weeks:
- Tumor Resection: Collection of a tumor portion (≥ 1-3 g) containing TILs.
- Isolation and Ex Vivo Expansion: TILs are extracted and cultured with IL-2 and irradiated feeder cells for rapid expansion (up to 10¹⁰ cells).
- Lymphodepletion: Administration of cyclophosphamide and fludarabine to create a favorable lymphocytic space.
- Re-injection: Infusion of expanded TILs, followed by high-dose IL-2 to stimulate their persistence.
- Monitoring: Surveillance for responses and toxicities (cytokine release syndrome, neurotoxicity).
Applications and Indications
TILs are primarily indicated for solid tumors refractory to standard treatments:
- Advanced Melanoma: Approved indication for lifileucel in patients who have progressed after checkpoint inhibitors and targeted therapy (if BRAF/MEK mutated). Objective response rate (ORR) of 30-50%, with 20% durable complete responses.
- Other Solid Tumors: Ongoing or promising trials for non-small cell lung cancer (NSCLC), cervical cancer, cutaneous squamous cell carcinoma (cSCC), Merkel cell carcinoma (MCC), and head and neck cancers.
In 2026, lifileucel shows efficacy in advanced NSCLC (IOV-LUN-202 trial), and real-world data support its early use in melanoma.
Recent Advances in 2026
The year 2026 marks a consolidation of clinical data:
- Real-World Data: Lifileucel (Amtagvi) confirms durable responses and improved survival in early advanced melanoma treatment.
- Pivotal Trials: Expected completion of recruitment for IOV-LUN-202 (NSCLC) and progression of TILVANCE-301 (Phase 3 frontline melanoma). Trial NCT07288073 for cSCC and MCC.
- Innovations: Development of neoantigen-specific TILs (NEO-STIM) and genetically modified versions (IOV-5001, IND expected early 2026) to improve persistence and reduce toxicity.
- Expanded Approvals: Approval in Canada for melanoma; European extension underway.
These advances position TILs as a viable option for immunologically "cold" solid tumors.
Major Challenges
- Logistical Complexity: Requirement for tumor resection and centralized production (4-6 weeks), limiting access.
- Toxicities: Cytokine Release Syndrome (CRS), neurotoxicity, and IL-2 side effects (hypotension, fever) in 70-90% of patients.
- Variable Efficacy: Durable responses in 20-30% of patients; lower efficacy in tumors with low mutational burden.
- Costs: Exceeding 500,000 euros per treatment, with regulatory challenges for multiple indications.
Future Perspectives
By 2030, TILs could integrate combinations with checkpoint inhibitors, "off-the-shelf" allogeneic TILs, or genetic modifications (CRISPR) to target more aggressive solid tumors. Ongoing trials and real-world data could lead to expanded approvals, reducing mortalities in advanced cancers by 15-25%. In France, the 2026-2030 Cancer Plan and European initiatives support access to these innovative therapies.
This report relies on data updated as of February 15, 2026. For a personalized clinical evaluation, please consult an oncologist specializing in immunotherapy.








